Quality Improvement Partners
This category is for website development and improvement for QIPstart

At Number 20. We don’t need another hero – Tina Turner
Tina letting us know that healthcare improvements are far better in multi-disciplinary teams. Those inspiration figures leading without coaching support can sometimes lead to unstainable improvements. And what happens when they leave?
In at 19… You’re So Vain by Carly Simon
Carly has seen a few of these. The leader/team manager who ‘knows it all’, keen to shoehorn their ‘experienced views’ whilst ‘practicing’ improvement. Often lacking a few key coaching skills
Breaking through at No 18. On My Own, By Pattie LaBelle and Michael Mcdonald
That training curriculum deadline looms. Not got time to get an improvement team together, too embarrassed to join a team so late? Nothing like doing a low-hanging fruit unstainable QI by yourself, As Pattie says ‘this wasn’t how it was supposed to be.’
In at 17. I heard it through the grape vine, by the legendary Marvin Gaye
All too common this one. Marvin in his own unique way describes the risk of relying on anecdotes and hearsay to formulate improvement aims. No proper measurements at baseline either. Oh no!
At 16, Thinking Out Loud, its Mr Ed Sheeran!
In the charts for a while now… Ed knows that it is important to brainstorm so to ‘understand the problem’ better. When not playing his guitar, he has a secret stash of sticky notes for a quick process map or fishbone to use with his improvement team.
Staying at 15, More than words, Extreme.
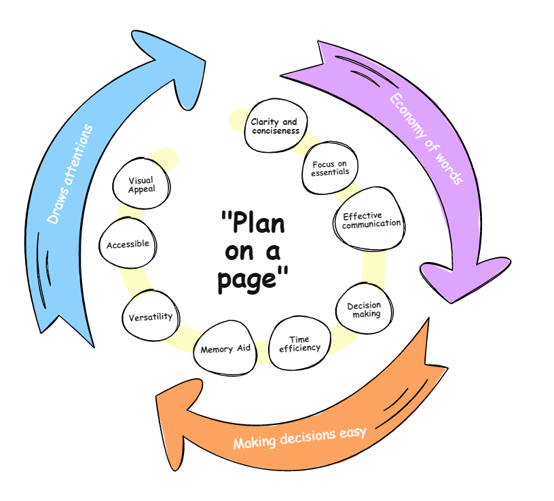
Don’t write pages when a few will do. Show your understanding, designs and measurements with a few choice improvement figures and run charts. Put it all together in an A3! It may engage more people than a business unit report…
A solid 14 for… Islands In The Stream, Kenny Rogers and Dolly Parton
Kenny and Dolly talk about the importance of sharing and scaling improvements properly through well designed quality management systems. Just how many isolated ward based sepsis programmes does a Trust need?
At 13, Livin’ on a Prayer, Bon Jovi.
Yep, you guessed it, random unevidenced interventions. Playing whac-a-mole until something sticks, usually under the cloud of operational pressures. Definitely ‘Livin’ on a prayer’.
Falling sharply at Number 12. Money for Nothing. Dire Straits.
Dire Straits wants you to know about starting small with your PDSAs. Don’t waste staff time and money on large scale PDSAs from the outset. Unless you want to print out 500 copies again of the wrong proforma again. There goes the budget!
Another steep drop at 11. Another one bites the dust by Queen
Freddie Mercury tells us of those Plan-Do-Study-Act cycles, where we just keep abandoning ideas because they ‘haven’t worked’. Forgetting to predict what happens in the planning phase, not taking the time to study or learn from each PDSA cycle.
Clinging on to No 10. Sitting on the dock of the bay by Otis reading
Otis is looking back on all those procrastinators and perfectionists who seem to take an eternity to move their improvements forward. Waiting for their data to come through (not SMART!), or waiting for that all important improvement team meeting in 3 months…
Up to Number 9. Shake it off by Taylor Swift.
Taylors in on it too. Just like in the Survivor track. No PDSA is a ‘bad’ PDSA. So if the PDSA doesn’t meet your prediction, learn from it and ‘shake it off’.
Straight in at number 8. Eye of the Tiger. Survivor
Put on this banging track to keep you working towards your improvement aim. Filled with resilience and perseverance, you may have some set backs, but with all that learning, you and your team will get there!
Going up to 7. Another Brick in the Wall. Pink Floyd
Pink Floyd appreciates that some improvements face many obstacles. The trick is to remove one brick at a time by breaking larger problems into smaller ones.
Falling at Number 6. The only way is up. Yazz and The Plastic Population.
We’ve all been there, those serial baseline measurements values were even lower than expected. But on the plus side, this leaves more scope to improve. Over to you Yazz!
Coming up to 5… Counting Stars by One Republic
This band knows that if you don’t measure you cannot say you have improved. They do acknowledge however that counting stars may not meet the ‘relevance’ criteria in as a healthcare SMART measurement.
Strong showing at No 4. Tow out of three ain’t bad by Meat Loaf.
Meat Loaf gets ‘very angry’ with those improvers who set challenging improvement aims from a baseline of 20% all the way to 100% in one go, in complex healthcare environments. He says set achievable expectations. Get from 20% to a new baseline of 66%, as Meat Loaf says ‘Two out of three ain’t bad’. You can always set a new improvement aim in the future.
Staying high at number 3… Levitating by Dua Lipa
Dua understands that a trend upwards of 7 consecutive measurement points in a row rarely happens by chance! The probability of that happening is 1 in 128!
Go Dua!
At number 2. I’ll Stand by you. The Pretenders,
Last week’s number one song. Through thick and thin, your improvement coach will stand by you. Fail fast, learn quick. Don’t give up. No doubt, a coach who loves their job can guide you through the whole improvement experience.
Up one place to Number 1, we have… Take a Bow by Madonna.
Madonna wants to celebrate with you! A true improvement team effort. All the stakeholders involved (including patients), a real attempt to understand the problem, clear aims and SMART measurement, using PDSA for learning. Sustaining over time, evidenced with data. All under the umbrella of continuous improvement. Take a bow!
I
=
In the project information section.
You will enter the Key Project Details, Identify who is in your QI team. There is also a QI team meeting log. To capture notes of activity outside PDSA.
In the Identify the Problem section
You will describe what it is like currently and expand on the reason for action of the problem identified. There is a tool to capture which people will be important to engage with using a stakeholder matrix.
In the Understand the Problem section
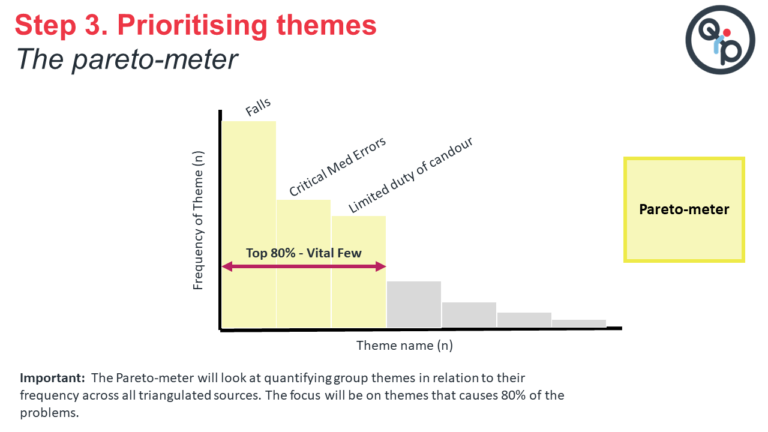
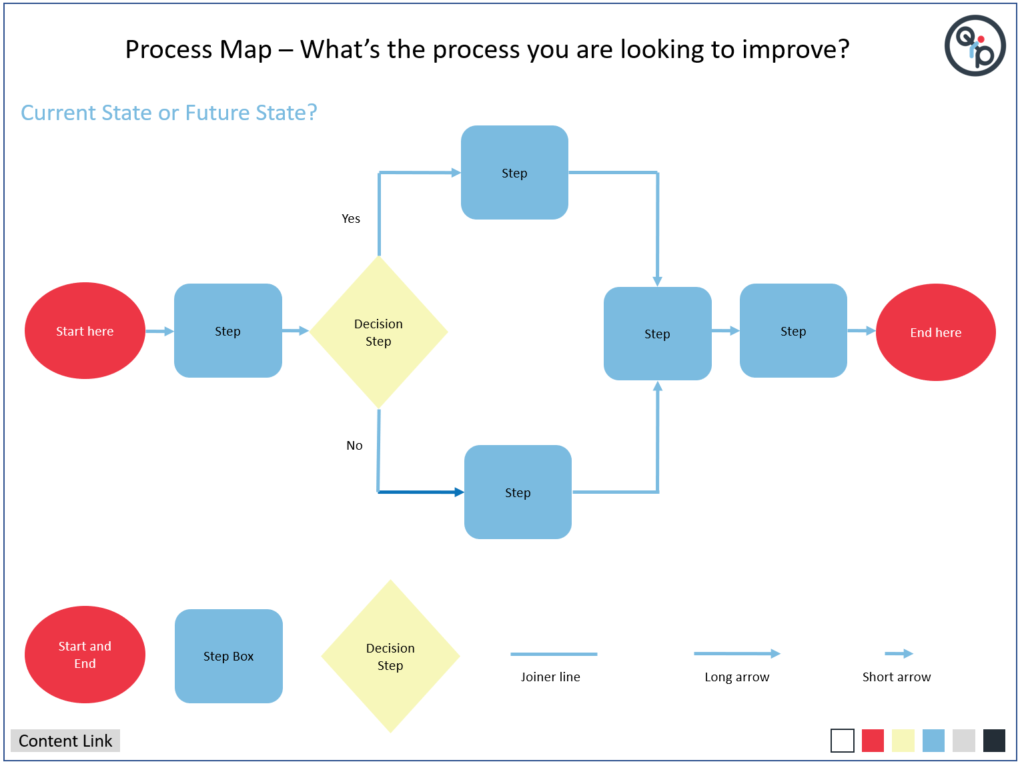
You will access to three of the most common tools that help to understand the problem better. These include Fishbone Diagram, a process map tool and finally a directly editable Pareto chart.
In the Design the Improvement Section
You will be prompted to expand on some key design questions. You will be asked to put in a SMART Aim and make a decision of what to measure and explain clearly how you will measure.

In the Deliver the Improvement Section
You will be given the tools to record your PDSA cycles and capture the measurements using run charts for outcome, process and balancing measures. Just duplicate the pages to add more run charts!
To change the data on the graph, it is just a simple case of [RIGHT CLICK] and scroll to ‘Edit Data’.
In the Sustain the Improvement Section
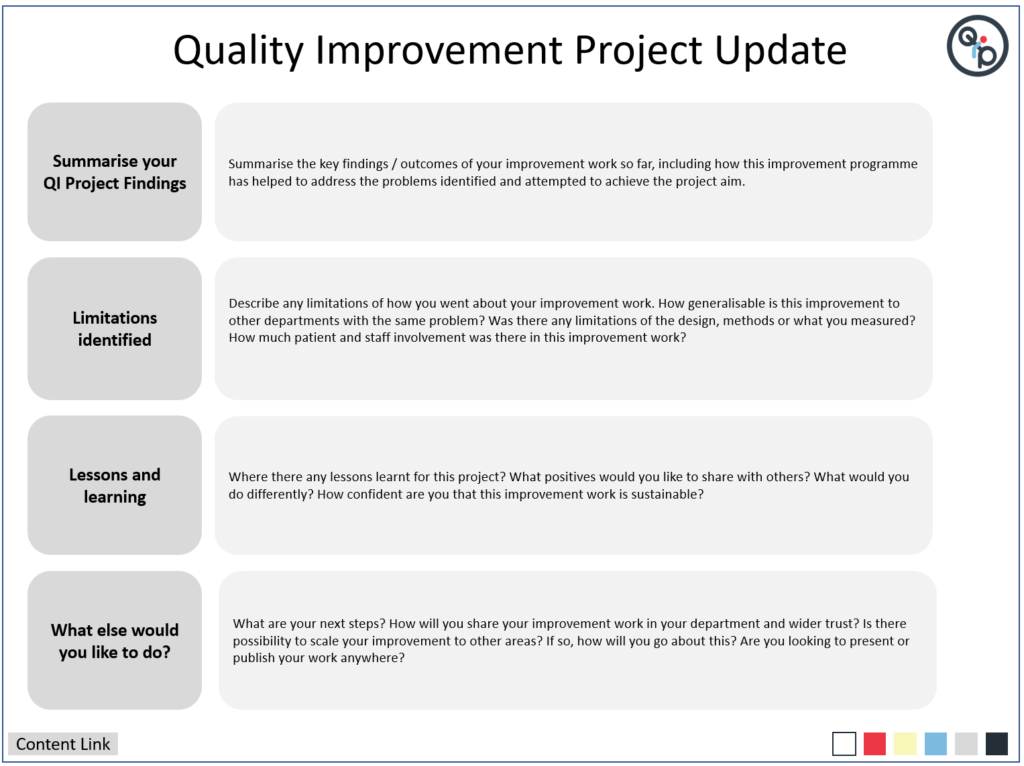
You will be asked to describe how you will sustain your improvement and an opportunity to provide a QI project update. this could be used as a handover document or to share with other the progress of your work so far. Remember some projects don’t ever finish as we are continually improving. So an update is all we need, rather then say we have ‘completed’ it
I

QI Method
What is it?
Breakthrough Collaboratives

Breakthrough Collaboratives, led by the Institute for Healthcare Improvement (IHI), are focused, time-limited initiatives that bring together healthcare organisations to achieve rapid and substantial improvements in specific and pre-determined areas of healthcare quality and safety. Participating organizations collaborate, learn from one another, and implement changes to address common challenges. They use data, structured learning, and peer networking to accelerate improvements. The aim is to achieve significant, large-scale changes that benefit patient care and safety with a focus on spreading successful strategies to other organizations and sustaining improvements over time.
Learn More: https://www.ihi.org/resources/Pages/IHIWhitePapers/TheBreakthroughSeriesIHIsCollaborativeModelforAchievingBreakthroughImprovement.aspx
Clinical Audit

Clinical audit helps to align care and benchmark against known standards, enhance patient safety, and ensure efficient and effective healthcare delivery. Clinical audit involves evaluating clinical practices, identifying areas for improvement, implementing changes, and monitoring progress. Key steps include defining objectives, collecting and analysing data, identifying discrepancies, making recommendations, implementing changes, and continuously reviewing and learning from the process.
Learn more: https://www.hqip.org.uk/wp-content/uploads/2018/02/developing-clinical-audit-patient-panels.pdf
Experience based co-design
Experience-based co-design (EBCD) is a collaborative approach used in healthcare service design, involving patients, staff, and families. It identifies issues in healthcare delivery, hosts co-design workshops to brainstorm solutions and iteratively tests and refines these solutions. EBCD emphasizes a patient-centred culture. It transforms healthcare by integrating patient and staff feedback to enhance care quality and satisfaction.
Learn more: https://www.pointofcarefoundation.org.uk/resource/experience-based-co-design-ebcd-toolkit/step-by-step-guide/1-experience-based-co-design/
Lean
Lean is a management philosophy and methodology that originated from manufacturing and has since been applied to various industries, including healthcare. It focuses on eliminating waste, improving efficiency and maximising value for customers or patients. Key principles of lean include identifying and reducing non-value-added activities, continuous improvement, empowering employees to contribute to problem-solving and creating a culture of efficiency and quality. Lean techniques, such as value stream analysis, 5S (Sort, Set in order, Shine, Standardize, Sustain), and Just-in-Time production are used to streamline processes and enhance productivity. Lean aims to deliver higher quality outcomes while reducing costs and resource waste.
Learn More: https://www.lean.org/explore-lean/what-is-lean/
Learning from Excellence

‘Learning from Excellence’ is a healthcare quality improvement approach that focuses on studying and extracting lessons from instances of excellence and exceptional care within the healthcare system. Unlike traditional quality improvement methods that primarily emphasize analysing errors and adverse events (often referred to as “safety I”), “Learning from Excellence” shifts the focus to understanding and replicating what goes right in healthcare delivery (often referred to as “safety II”).
Learn More: https://learningfromexcellence.com/about/
Learning from Incidents

‘Learning from incidents’ begins with prompt incident reporting and thorough analysis to identify root causes and contributing factors. From this analysis, actionable recommendations for improvement are formulated and implemented, including adjustments to protocols, training enhancements, or equipment upgrades. Continuous monitoring ensures that changes lead to improved emergency responses, while knowledge sharing fosters a culture of improvement. Ongoing training is provided based on incident findings, and protocols are regularly reviewed and adapted to address emerging challenges, ensuring that service remains responsive and effective in delivering critical care.
Learn more: https://qualitysafety.bmj.com/content/26/3/252
Model for Improvement

The Model for Improvement is a framework used to systematically improve processes. It involves asking three key questions: What are we trying to accomplish (Aim)? How will we know a change is an improvement (Measures)? What changes can we make to achieve improvement (Interventions)? And then uses a four-step cycle in an iterative approach to work towards the aim set: Plan (identify and plan changes), Do (implement changes on a small scale), Study (analyse results), and Act (decide whether to adopt, adapt, or abandon changes).
Learn More: https://www.ihi.org/resources/Pages/HowtoImprove/default.aspx
Operational Excellence / Quality Management System (QMS)

A Quality Management System (QMS) is a structured framework within an organization to consistently meet or exceed patient expectations and adhere to quality standards. Quality Management systems are becoming more popular within the healthcare sector and typically consist of several key components:
Quality planning – Collectively agreeing what the overall System (or organisation) wants to deliver and how to do this
Quality Assurance – checks which are put in place to ensure quality of care is being delivered using verified evidence and articulating improvements which have bene made, or areas for further focus
Quality Control – the way monitoring and maintenance occurs to ensure that we know whether the system is achieving the outcomes required
Quality Improvement – the systematic approach used to make tangible change and improve performance
This draws heavily on Lean methodology, adapted for healthcare.
Learn More: https://kpmg.com/xx/en/home/industries/healthcare/operational-excellance-in-healthcare.html
QSIR

QSIR, which stands for “Quality, Service Improvement, and Redesign,” is a comprehensive healthcare approach aimed at improving patient care and outcomes. This is a dedciated set of training courses (depending on your experience) and repository of tools and techniques which can be used to enhance quality standards, streamline service delivery for efficiency and effectiveness, and foster innovative process redesign. Utilising tools such as process mapping and improvement cycles like Plan-Do-Study-Act (PDSA), QSIR promotes a consistent understanding of QI tools which can be used and aims to standardise QI in the NHS.
Learn More: https://aqua.nhs.uk/QSIR/
Six Sigma

Six Sigma is a data-driven approach used for process improvement and quality management across various industries. It aims to reduce process variations and defects, ensuring consistent high-quality outcomes. Six Sigma follows a structured approach known as DMAIC (Define, Measure, Analyse, Improve, and Control) and emphasizes data-driven decision-making, customer focus, and continuous improvement. Trained professionals, known as Black Belts and Green Belts, lead and support improvement projects. The ultimate goal is to enhance quality, reduce costs, and achieve customer satisfaction through empirical evidence and ongoing optimisation.
Learn more: https://www.youtube.com/watch?v=4EDYfSl-fmc&ab_channel=Simplilearn
Toyota Kata

Toyota Kata is a structured improvement and coaching routine developed by Toyota. It involves understanding the current condition, setting a target condition, experimenting, and iterating toward improvements. Leaders provide direction and challenges, while the Improvement Kata and Coaching Kata routines guide teams through the problem-solving process. The PDCA (Plan-Do-Check-Act) cycle is integral to the approach, and a fundamental principle is the respect for people, encouraging collaboration and shared responsibility for continuous improvement.
Learn More: http://www-personal.umich.edu/~mrother/Homepage.html
Virginia Mason Improvement Approach

Virginia Mason’s improvement approach, often associated with the Virginia Mason Production System (VMPS), is a healthcare approach that focuses on continuous improvement, patient safety, and delivering high-quality care. Key elements of this approach include a patient-centric culture, Lean principles, and interdisciplinary teamwork. It aims to streamline processes, eliminate waste, engage staff, and enhance patient experiences. This draws heavily on Lean methodology, adapted for healthcare.
Learn More: https://www.virginiamasoninstitute.org/resource/case-study-bringing-impact-within-reach/
Hi Everyone, this week we will try something different!

Steve has a busy night in the Minecraft Emergency Department. On his way home he wonders if there is a better way of doing thing…

He stumbles upon this big sign saying QI. What appears beyond it looks like a big castle with a tall tower. His natural curiosity takes him to castle entrance.

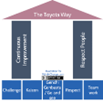
He sees signs for Model for Improvement. The tower looks like it has 3 floors, each asking a question and some large letters made of Minecraft blocks on the roof. Of course, he is off to climb the stairs.

The roof has the letters P D S A . One letter for each quadrant. In each bay there are smaller signs that explain the important things to remember for Plan, Do, Study and Act

Steve also finds out that simply knowing about Model for Improvement and PDSA will not be enough, there are other things he will need to understand to strengthen his armour and do improvement well.

Steve feels ready to have a go. He knows that he can only get better with practice. In the next video he will try to use the 3 questions and cycles of PDSA for his first improvement mission. Make sure you tune in!

In this week’s blog, I would like to share two podcasts describing how as a member of clinical staff you might get started with QI. I was interviewed by Rachel Saville from medical education podcast site MemCast. She also is a Respiratory Trainee Registrar in East Midlands area. Thanks Rachel! I hope you find them enjoyable. There are plenty of tips and insights for new clinicians who are beginning their QI journey. The content and links to the podcasts are described below.